The recent budget marks 12.93% hike in the health sector budget compared to last year’s budget of 2023-24. The paucity of health workers in the country is, unfortunately, underpinned by a lackadaisical attitude towards recruitment and retention fails to ensure empathy-based maternal care. In India, highest proportion of pregnancies are classified as high-risk pregnancy where clean specialist care is needed to reduce risk of complications endangering lives of mother with neonates. It is this existing state of disparity in maternal health outcomes among urban, rural and tribal populations which further contributes to making it worst. Through this article, we try to highlight the not so pleasant situation of maternal health in India specifically looking at urban, rural and tribal communities.
Maternal Health in the Urban India
Compared with rural and tribal areas, urban areas in India have better access to health care services because of which a relatively small but significant improvement was noted regarding maternal health indicators. Focus group discussions suggested that the MMH care utilization rate decreased instead accepting payment from other attention dependents increased. But in urban areas, the rate of high-risk pregnancies is very high.
Key Data:
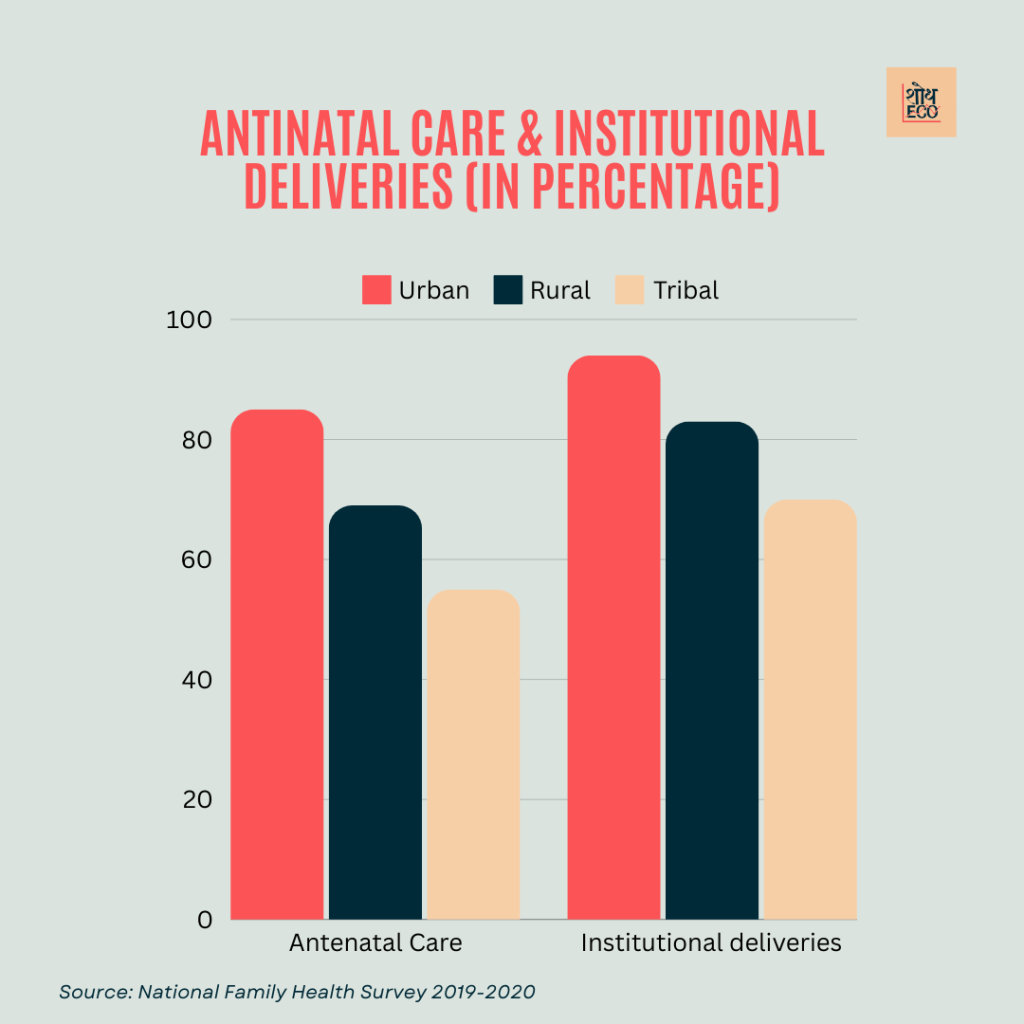
Antenatal Care (ANC): NFHS-5 2019–2020 reports at least four ANC visits to a staggering 85% of pregnant women in urban areas.
Institutional Deliveries: About 94% of the births take place in healthcare facilities and across urban areas.
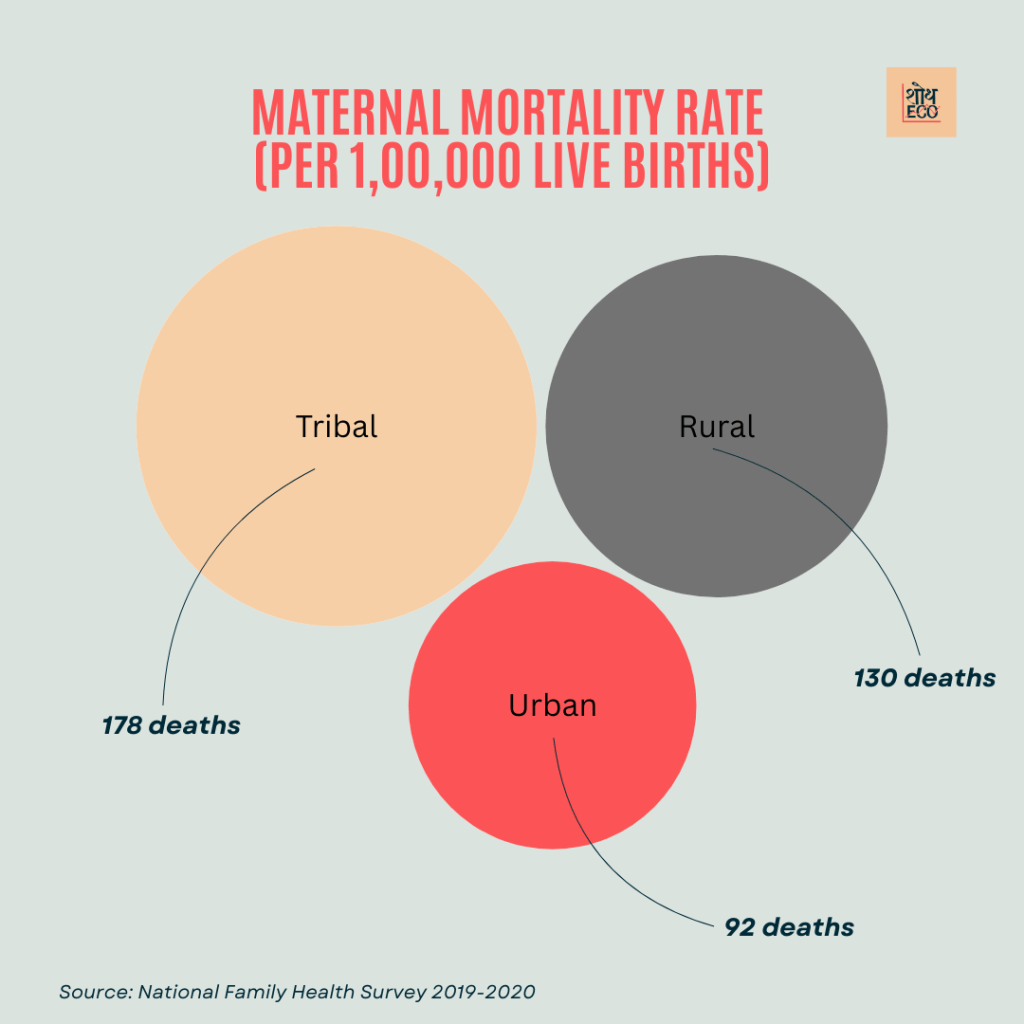
Maternal Mortality Ratio (MMR): It is around 92 deaths per 100,000 live births in urban India.
Urban bodies report higher rates of gestational diabetes, hypertension and advanced maternal age leading to high risk pregnancies.
Even though these are good signs, there are also overcrowded hospitals in cities and sub-optimal maternal health services for those living in slums who require personalized care. Accessing quality maternal healthcare is a challenge in slum areas of the cities due to which urban poor are subjected to higher rates of maternal morbidity and mortality.
Maternal Health In Rural Area
The major challenge as far as rural areas are concerned (they comprise close to 65% of the population with regard to India) is in striving towards improving maternal health. This creates severe obstacles because health services are scarce, and there is a high rate of existing high-risk pregnancies.
Key Data:
Antenatal Care (ANC): Complete four or more visits of ANC attended percentage among pregnant women in rural area were 69 %.
Delivery in Institutional at Facilities: Approximately 83% of rural births.
Maternal Mortality Ratio (MMR): The MMR is higher in rural India, which stands around 130 deaths per 1000,00 live births.
High Risk Pregnancies: In rural areas however factors like anemia, malnutrition & inadequate prenatal care makes the pregnancies high risk.
Such an environment is only made worse by the scarcity of trained healthcare professionals, poor infrastructure facilitating high maternal and infant deaths rates as well as difficult to use transportation systems. Progress has been made over the years by government initiatives such as Janani Suraksha Yojana (JSY) and Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) in tackling rural maternal health, yet large gaps persist.
Tribal Health in India– Maternal Community and Public provider Perspective
Maternal health disparities are the most pronounced among tribal populations, 8.6% of India‘s population. Other causative agents for high-risk pregnancies (including malnutrition, lack of access to quality care and cultural practices) are common there.
Key Data:
Antenatal Care (ANC): There was also a significant gap in the proportion of at least four ANC visits by pregnant women — 55% for tribal areas.
Institutional Deliveries: 70% of tribal area born in healthcare facilities.
Maternal Mortality Ratio (MMR): The MMR is too high in tribal areas, expected to be around 178 deaths per every one lakh live births.
High-Risk Pregnancies (due to high incidences of anemia, malnutrition and limited access to emergency obstetric care)
These regions are characterized by cultural barriers, geographical isolation and scarcity of healthcare facilities which results in a lower maternal health outcomes. While the government and NGOs like Tribal Health Care Research Programme are trying hard to turn around these grim statistics yet grave challenges remain.
Conclusion
The high rate of HRPs in India together with an increased risk for maternal deaths indicate the importance to focus on intervention strategies targeted towards ameliorating maternal health especially in rural, tribal areas. Relatively urban areas present better maternal health indicators, but the poor in these settings encounter large barriers. Rural and tribal regions need major healthcare access improvements, infrastructure investments as well as culturally-sensitive care delivery.
The disparity to these needs calls for a comprehensive solution approach that involves building of the healthcare infrastructure, training more healthcare providers, transport and referral systems improvements among others as well improving community based maternal health. By affording a maternal health focus throughout all demographics, India can provide robust mothers and children and overall have better national good health.
